 Jun, 17 2026
Jun, 17 2026
An expired vial of critical medication in an ICU isn't just a waste issue-it's a potential safety crisis. When life-saving drugs like vasopressors or neuromuscular blockers hit their expiration date, you can't simply wait for the next shipment. You need a structured way to decide who gets treated first and with what alternative. This is where medication replacement prioritization becomes your most vital tool.
In healthcare settings, especially intensive care units (ICUs), patients rely on complex regimens that change daily. A study published in PMC (2023) highlights that medication is the most common intervention for ICU patients. If you handle replacements poorly, you risk polypharmacy errors, inappropriate continuation of acute meds, or failure to restart chronic ones. These mistakes contribute to early unplanned hospital readmissions, which occur at an 11-12% rate within 30 days. The goal here is clear: keep patients safe while managing limited resources efficiently.
Why Expiration Dates Matter More Than You Think
We often treat expiration dates as rigid deadlines, but in critical care, they signal a shift in availability. The FDA reported 136 medications in shortage as of April 2024, showing how systemic these issues are. While shortages and expirations are different triggers, the response framework is identical. According to the American Society of Health-System Pharmacists (ASHP), organizations must have clear protocols for therapeutic alternatives when standard meds become unavailable.
The problem? Many hospitals still use ad hoc methods. During the remdesivir shortage, 47% of hospitals used a "first come, first served" approach, and 22.7% used random lotteries. Only 4.5% considered comorbidities. This inconsistency creates inequities. Without a standardized protocol specifically for expired critical medications, institutions scramble, leading to dangerous substitutions or delays. The ASHP Guidelines on Managing Drug Product Shortages (2023) provide the backbone for fixing this, emphasizing evidence-based tiering over guesswork.
The Three-Tier Framework for Alternatives
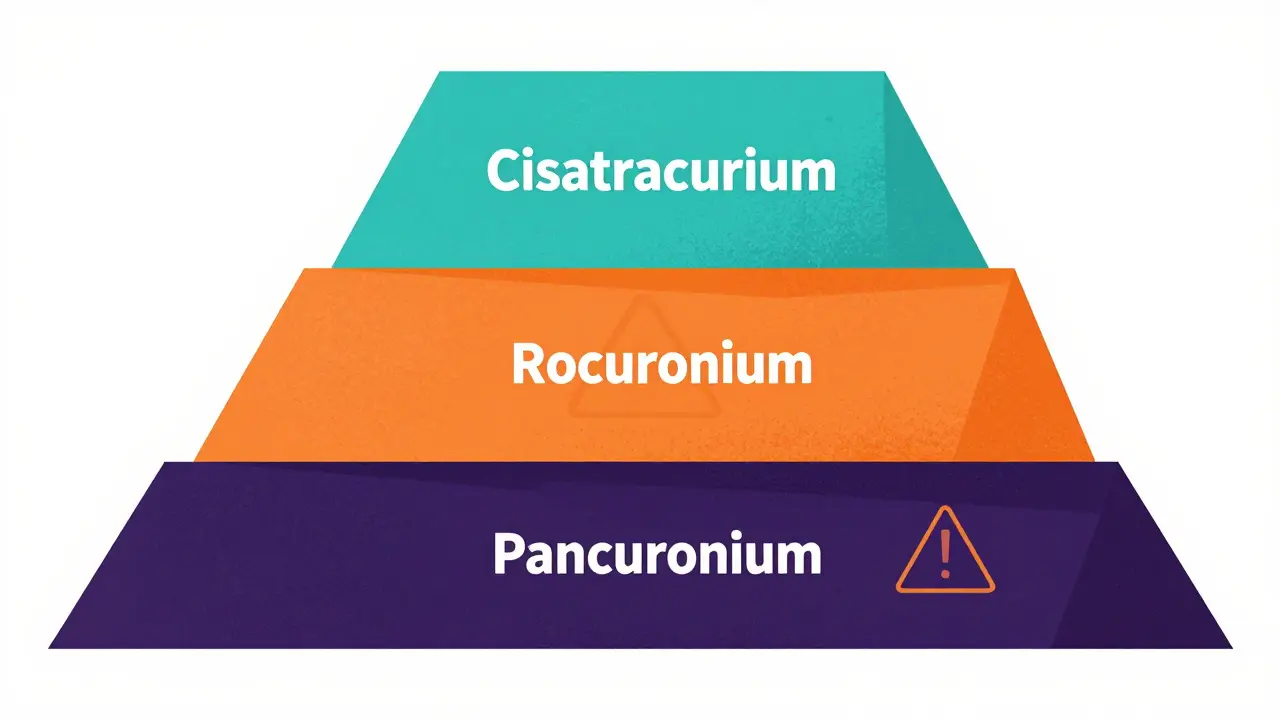
When a critical med expires, you don't just pick any substitute. You follow a tiered system. The ASHP resource document 'Considerations for Prioritizing Medications for Mechanically Ventilated Patients' outlines this clearly. Let’s look at neuromuscular blocking agents as an example:
- 1st Line: Cisatracurium (preferred due to stability and side effect profile).
- 2nd Line: Rocuronium or Vecuronium (effective but may require dose adjustments).
- 3rd Line: Atracurium or Pancuronium (used only if others are unavailable, requiring closer monitoring).
This isn't a one-size-fits-all list. Pharmacists must assess individual patient needs. For instance, renal function might make cisatracurium ideal, while hepatic issues could shift preference. The key is adjusting doses based on patient response and clinical course. Monitoring parameters like the Richmond Agitation-Sedation Scale (RASS) scores ensures sedation remains effective without oversedating. This structured approach prevents therapeutic inequivalence-the risk that the substitute doesn't work as well as the original.
| Tier | Medication | Key Consideration | Monitoring Need |
|---|---|---|---|
| 1st Line | Cisatracurium | Hofmann elimination (organ-independent) | Standard RASS |
| 2nd Line | Rocuronium | Hepatic metabolism | Liver function tests |
| 3rd Line | Pancuronium | Cardiac effects possible | Continuous ECG |
The Seven-Step Implementation Process
Executing this plan requires discipline. The ASHP guidelines outline a seven-step process that turns chaos into order:
- Validate Expiration Details: Confirm quantity, expiration date, and criticality level.
- Determine Stock on Hand: Check inventory systems for remaining unexpired stock.
- Identify Affected Populations: Which patients are currently receiving this med? Who will start soon?
- Identify Therapeutic Alternatives: Use the tiered system above to select substitutes.
- Conduct Financial Impact Analysis: Evaluate cost differences between primary and alternative agents.
- Implement Information System Changes: Update bar coding, order sets, and pharmacy databases.
- Establish Monitoring Protocols: Define how success will be measured (e.g., withdrawal symptoms, efficacy).
This process takes time-typically 8-12 hours of interdisciplinary team effort for critical scenarios. Pharmacists spend about 45 minutes per patient evaluating alternatives, according to CU Anschutz research (August 2025). It’s not fast, but it’s safe. Skipping steps leads to errors. For example, failing to update information systems can result in nurses administering expired drugs by mistake.
The Role of Pharmacists in Crisis Management
Pharmacists are the engine of this process. Dr. Sikora of CU Anschutz states, "Critical care pharmacists provide an essential cognitive service in the form of comprehensive medication management (CMM)." In 2025, national guidelines published in Pharmacotherapy confirmed that pharmacist-run CMM reduces mortality by 18.7% and shortens ICU stays by 2.3 days across 10,000 cases. That’s not optional; it’s standard of care.
However, access varies wildly. Academic medical centers report 89.3% adoption of formal protocols, while community hospitals sit at 42.1%. Why? Resource constraints. 68.4% of community hospitals lack adequate medication management resources. Dr. Mark Reynolds, a community intensivist, noted on Reddit (January 2025): "Without dedicated critical care pharmacists, we're forced to use less optimal alternatives... leading to 3 medication-related complications last quarter." This gap highlights a systemic vulnerability: expertise saves lives, but it’s unevenly distributed.

Real-World Challenges and Success Factors
Let’s talk reality. Sarah Chen, an ICU pharmacist at University of Michigan Health System, shared her experience on the ASHP Community Forum (November 2024): "When our fentanyl supply expired unexpectedly last winter, we spent 72 hours transitioning 14 ventilated patients to hydromorphone alternatives while monitoring for withdrawal symptoms-having the ASHP tiered guidance saved us from making dangerous substitutions." Her story underscores two points: preparation matters, and expert oversight prevents harm.
Common challenges include insufficient time (reported by 63.2% of respondents in the 2024 Medication Safety Report), unclear guidelines (48.7%), and communication breakdowns (39.4%). High-performing institutions solve this with:
- Daily Interdisciplinary Reviews: Implemented in 76.4% of top-quartile hospitals.
- Automated Inventory Tracking: Systems providing 30-day expiration alerts are used by 68.2% of institutions with <5% expired medication incidents.
- Pre-Established Pathways: Alternative therapy pathways exist in 78.3% of high-reliability organizations.
These aren’t luxuries; they’re necessities. Automated alerts give you lead time. Pre-established pathways remove decision fatigue during crises. Daily reviews ensure no patient falls through the cracks.
Future Trends and Regulatory Pressure
The landscape is shifting. The global medication safety technology market grew to $3.27 billion in 2024, projected to reach $7.89 billion by 2029 (Grand View Research). Regulatory bodies are watching closely. The Joint Commission cited medication management in 68.4% of sentinel events in 2024, up from 59.2% in 2022. CMS reimbursement penalties now affect 22.4% of hospitals for medication-related readmissions exceeding 15%.
New developments offer hope. The FDA’s April 2025 draft guidance on 'Optimizing Medication Expiration Dating' proposes standardized stability testing, potentially reducing unnecessary waste by 18-22%. Meanwhile, CU Anschutz researchers are piloting an AI-driven substitution system analyzing 147 patient variables, showing 94.7% concordance with expert recommendations. By Q1 2026, updated ASHP guidelines will specifically address expired medications, distinct from general shortages. This evolution promises greater standardization, but only if we bridge the pharmacist shortage gap-projected to hit 112,000 vacancies by 2027.
What should I do immediately when a critical medication expires?
First, validate the expiration details and check remaining stock. Then, identify affected patients and consult your institution’s tiered alternative list. Do not administer expired medication. Notify pharmacy and nursing leadership to initiate the replacement protocol.
Is it safe to use off-label alternatives for expired critical meds?
Yes, if guided by evidence-based protocols like those from ASHP. Off-label use is common in critical care shortages, but it requires careful dose adjustment and monitoring for adverse effects. Always document the rationale and obtain necessary approvals.
How can small hospitals manage this without dedicated pharmacists?
Small hospitals should establish telepharmacy partnerships or regional collaboration networks. Implement automated inventory alerts to gain lead time. Use pre-approved alternative pathways developed in consultation with external experts to reduce decision burden during crises.
What is the financial impact of poor medication replacement prioritization?
Poor prioritization leads to extended ICU stays, higher readmission rates, and potential CMS penalties. Studies show pharmacist-led management reduces ICU stay by 2.3 days on average, saving significant costs per patient. Conversely, errors can increase length of stay by over 11 days in some cases.
Will new FDA guidelines help reduce expired medication waste?
Yes. The April 2025 FDA draft guidance aims to standardize stability testing, which could extend shelf-life appropriately and reduce unnecessary expiration-related waste by 18-22%. This helps maintain stock levels and reduces frequency of replacement crises.