 Feb, 11 2026
Feb, 11 2026
When you're on Medicaid, getting your prescriptions filled shouldn’t be a guessing game. But many people don’t know what’s actually covered - or what hurdles they might hit before they can get their meds. The truth is, Medicaid pays for most prescription drugs, but not all of them. And how much you pay? That depends on your state, your drug, and sometimes even your doctor’s notes.
What Drugs Does Medicaid Cover?
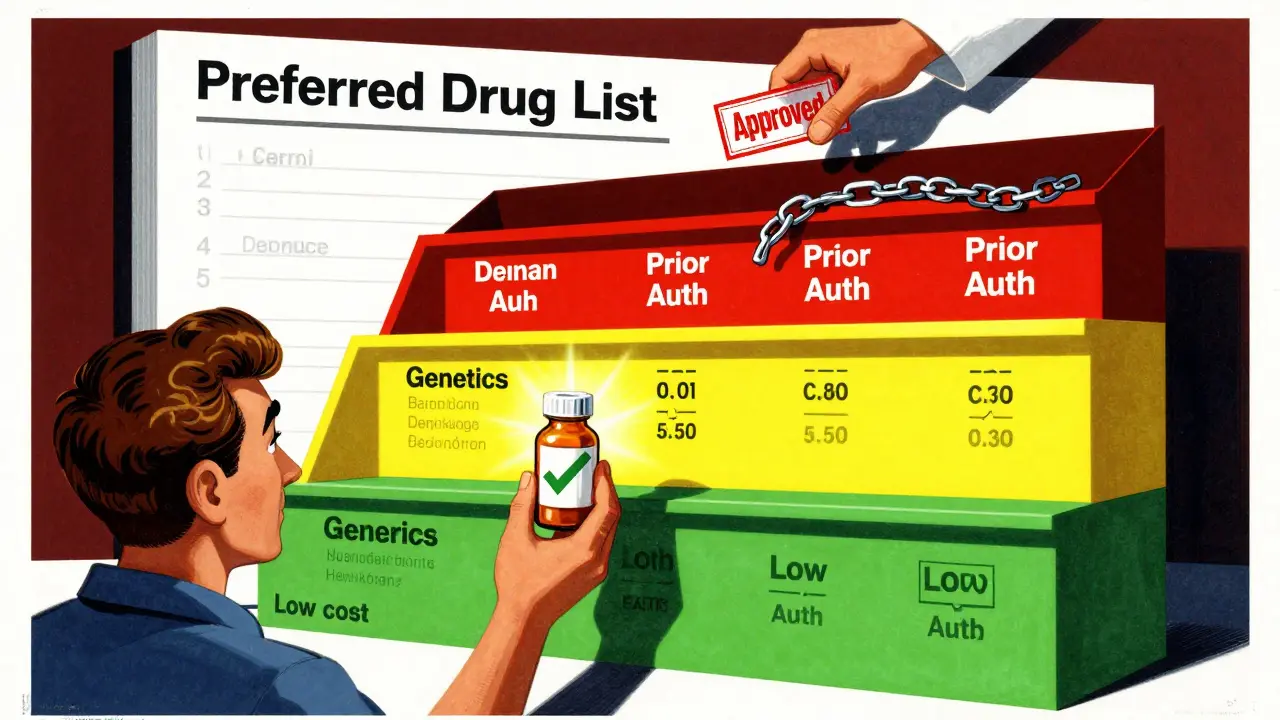
All 50 states and Washington, D.C., cover outpatient prescription drugs under Medicaid. That’s not optional - it’s standard. But here’s the catch: Medicaid doesn’t cover every single drug on the market. Each state builds its own list of approved medications, called a Preferred Drug List (PDL). This list decides which drugs are easy to get and which ones need extra steps.
Most states divide drugs into tiers. Tier 1 is usually generic drugs - the cheapest, most common versions. You’ll pay the least here, often just $1 to $5 per prescription. Tier 2 includes brand-name drugs that don’t have generics yet. These cost more - maybe $15 to $40. Then there are Tier 3 or Tier 4 drugs: specialty medications. These are for serious conditions like cancer, rheumatoid arthritis, or hepatitis C. They can cost hundreds or even thousands of dollars. Medicaid covers them, but only if you jump through hoops.
How States Decide What’s Covered
States don’t just pick drugs randomly. They use a Pharmacy and Therapeutics (P&T) committee - made up of doctors, pharmacists, and sometimes patients - to review which drugs offer the best value. They look at effectiveness, safety, and cost. If a cheaper generic works just as well as a brand-name drug, the state will push you toward the generic first.
That’s where step therapy comes in. If your doctor prescribes a drug that’s not on the preferred list, you might have to try two other drugs first. For example, if you need a new antidepressant but your state’s PDL lists three others as preferred, you’ll have to try those two first - and fail - before they’ll approve the one your doctor wants. This rule is called "trial and failure," and 38 states use it as of 2025.
Some states make exceptions. If you’re already on a drug that works, or if your condition is rare or life-threatening, you might skip the trial phase. But you’ll need documentation - usually a letter from your doctor explaining why the preferred options won’t work for you.
Prior Authorization: The Hidden Gatekeeper
Even if a drug is on the list, it might still need prior authorization. This means your doctor has to call or submit paperwork to your state’s Medicaid office before you can get the prescription filled. Common reasons for prior authorization include:
- High-cost drugs (like insulin pumps or biologics)
- Drugs with safety risks (like certain painkillers or antipsychotics)
- Drugs that are often misused (like opioids or benzodiazepines)
In North Carolina, for example, prior authorization for insulin used in Type 1 Diabetes can last up to three years - meaning once approved, you won’t need to reapply every time. But for drugs like Epidiolex (used for rare seizures), the state moved it from "preferred" to "non-preferred" in July 2025, making prior authorization mandatory. That doesn’t mean you can’t get it - it just means more paperwork.
On average, it takes 7.2 business days to get prior authorization approved. If you’re denied, you can appeal - and 78% of appeals succeed if your doctor includes detailed clinical notes. That’s why keeping good records matters.
What You Pay Out of Pocket
Cost-sharing varies by state and income level. Most Medicaid beneficiaries pay:
- $0 to $5 for generic drugs
- $10 to $45 for brand-name drugs
- Higher amounts for specialty drugs - but often capped
There’s also a big help program called Extra Help (or Low-Income Subsidy). If you qualify for full Medicaid, you automatically qualify for Extra Help with Medicare Part D. That means:
- $0 monthly premium
- $0 deductible
- Maximum $4.90 copay for generics
- Maximum $12.15 for brand-name drugs
- After you hit $2,000 in total drug costs for the year, you pay $0
Yet, nearly 1.2 million people who qualify for Extra Help don’t even know they’re eligible. If you’re on Medicaid, you’re likely already eligible - no separate application needed.
Where You Can Fill Your Prescriptions
You can’t just go to any pharmacy. Medicaid works with a network of approved pharmacies. Most states use big chains like CVS, Walgreens, or Walmart. Some also have mail-order services for maintenance medications - like blood pressure pills or diabetes drugs. Using mail order can cut your copay even further and ensure you never run out.
Always check if your pharmacy is in-network before you go. Out-of-network pharmacies might not bill Medicaid at all, leaving you with a $200 bill for a drug that should’ve cost $5.
What’s Not Covered - And Why
Medicaid doesn’t cover every drug you can think of. Here are common exclusions:
- Drugs for weight loss (like Ozempic or Wegovy) - unless used for diabetes
- Over-the-counter medications - even aspirin or antacids
- Drugs used for cosmetic purposes - like hair growth treatments
- Drugs not approved by the FDA
- Drugs removed from the formulary due to cost - like Vasotec, Trulance, or Vanos Cream, which North Carolina dropped in 2025 because they no longer qualified for federal rebates
States remove drugs when they stop getting rebates from manufacturers. That’s because Medicaid gets a discount on every drug it covers - the bigger the rebate, the more money the state saves. If a drug’s rebate drops below a certain level, it gets cut.

State Differences Matter - A Lot
North Carolina’s formulary is not Florida’s. Florida has a separate Quick Reference Guide for physician-administered drugs - things you get in a clinic, not a pharmacy. Texas might cover a drug that New York denies. That’s because each state negotiates its own contracts with pharmacy benefit managers (PBMs) like CVS Caremark, Express Scripts, or OptumRx.
North Carolina saved $127 million between 2010 and 2023 just by managing its formulary. But that savings came with trade-offs. Some patients had to wait longer for meds. Others had to switch drugs that worked fine - just because a cheaper one existed.
That’s why knowing your state’s rules matters. If you’re moving, check your new state’s PDL. If you’re struggling to get a drug, call your state’s Medicaid office - or find a local SHIP counselor. They help people navigate this stuff every day.
What’s Changing in 2025 and Beyond
Things are shifting fast. Starting in 2025, Medicaid beneficiaries can change their drug plans once a month - not just once a year. That’s huge. If a drug gets removed from your formulary, you can switch to a better plan without waiting.
The Inflation Reduction Act also capped out-of-pocket drug costs at $2,000 per year for Medicare Part D. Since many Medicaid users are dual-eligible (they get both Medicare and Medicaid), this means even less financial stress.
CMS is also updating its rules in early 2026. States will now have to prove their formularies don’t block access to medically necessary drugs. That could mean fewer denials and faster approvals.
But the big challenge remains: specialty drugs. New gene therapies cost over $2 million per dose. Medicaid programs are scrambling to find ways to pay for them without breaking the budget. Some states are now testing outcome-based contracts - where manufacturers only get paid if the drug works.
What You Should Do Right Now
Don’t wait until you’re denied a prescription to learn the rules. Here’s what to do:
- Find your state’s current Preferred Drug List. Search "[Your State] Medicaid Preferred Drug List 2025".
- Check if your drug is on it - and what tier it’s in.
- If it’s not preferred, ask your doctor if there’s a preferred alternative.
- If you need prior authorization, ask your doctor to submit it early - with full clinical notes.
- Use in-network pharmacies. Mail-order is often cheaper and more reliable.
- If you’re on Medicare too, confirm you’re getting Extra Help. It’s automatic if you have full Medicaid.
Medicaid covers a lot - but it’s not magic. It’s a system designed to balance access and cost. Knowing how it works is the best way to make sure you get what you need - without the delays, denials, or surprise bills.
Does Medicaid cover all prescription drugs?
No. Medicaid covers most prescription drugs, but each state has its own list of approved medications called a Preferred Drug List (PDL). Drugs not on the list may require prior authorization or step therapy. Some drugs, like over-the-counter medications or those used for cosmetic reasons, are never covered.
Why does my state require me to try other drugs first?
This is called step therapy or "trial and failure." States use it to control costs by encouraging the use of cheaper, equally effective generic drugs before approving more expensive brand-name or specialty drugs. It’s required in 38 states as of 2025, but exceptions exist for serious or rare conditions.
How much will I pay for my medications?
Most Medicaid beneficiaries pay $0-$5 for generics and $10-$45 for brand-name drugs. If you qualify for Extra Help (automatic if you have full Medicaid), your copays drop to $4.90 for generics and $12.15 for brands, with $0 after you hit $2,000 in annual drug costs.
Can I use any pharmacy with Medicaid?
No. You must use pharmacies in your state’s Medicaid network. Out-of-network pharmacies won’t bill Medicaid, and you’ll be responsible for the full cost. Check your state’s list or call your Medicaid office before going to a pharmacy.
What if my drug is removed from the formulary?
If your drug is removed, you may still get it through prior authorization if your doctor proves it’s medically necessary. Some states allow exceptions if you’re already taking the drug and it’s working. Contact your state’s Medicaid office or a SHIP counselor for help navigating the change.
Can I get help if I’m denied a prescription?
Yes. You can appeal a denial. If your doctor provides detailed clinical notes showing why the preferred drug won’t work for you, 78% of appeals are approved. Contact your state’s Medicaid office or a patient advocacy group like Families USA for guidance.
Do I need to reapply for Medicaid drug coverage every year?
No. Once you’re enrolled in Medicaid, your drug coverage continues as long as you remain eligible. However, your state’s formulary may change during the year, which could affect which drugs are covered or how much you pay. Stay informed by checking your state’s PDL updates.
Suzette Smith
February 12, 2026 AT 09:58Autumn Frankart
February 14, 2026 AT 07:28andres az
February 15, 2026 AT 23:16Stephon Devereux
February 16, 2026 AT 06:57steve sunio
February 16, 2026 AT 08:05Sonja Stoces
February 18, 2026 AT 07:59Rob Turner
February 19, 2026 AT 10:53Luke Trouten
February 20, 2026 AT 16:42Rachidi Toupé GAGNON
February 22, 2026 AT 05:08Gloria Ricky
February 23, 2026 AT 11:09Stacie Willhite
February 24, 2026 AT 13:56Jason Pascoe
February 24, 2026 AT 15:37Jim Johnson
February 24, 2026 AT 23:52christian jon
February 25, 2026 AT 07:13