 Dec, 8 2025
Dec, 8 2025
HIT Diagnostic Score Calculator
The 4Ts score helps doctors assess the probability of Heparin-Induced Thrombocytopenia (HIT). Enter your values for each criterion below.
Did platelets drop by more than 50% from baseline?
When did the platelet drop occur after starting heparin?
Are there new or worsening blood clots?
Could another condition explain the platelet drop?
When you're given heparin after surgery or for a blood clot, you expect it to protect you - not put you at risk for something worse. But for a small number of people, heparin doesn't just thin the blood. It triggers a dangerous immune reaction that causes platelets to crash and blood clots to form. This is heparin-induced thrombocytopenia, or HIT. It's rare, but when it happens, it can be life-threatening.
What Exactly Is HIT?
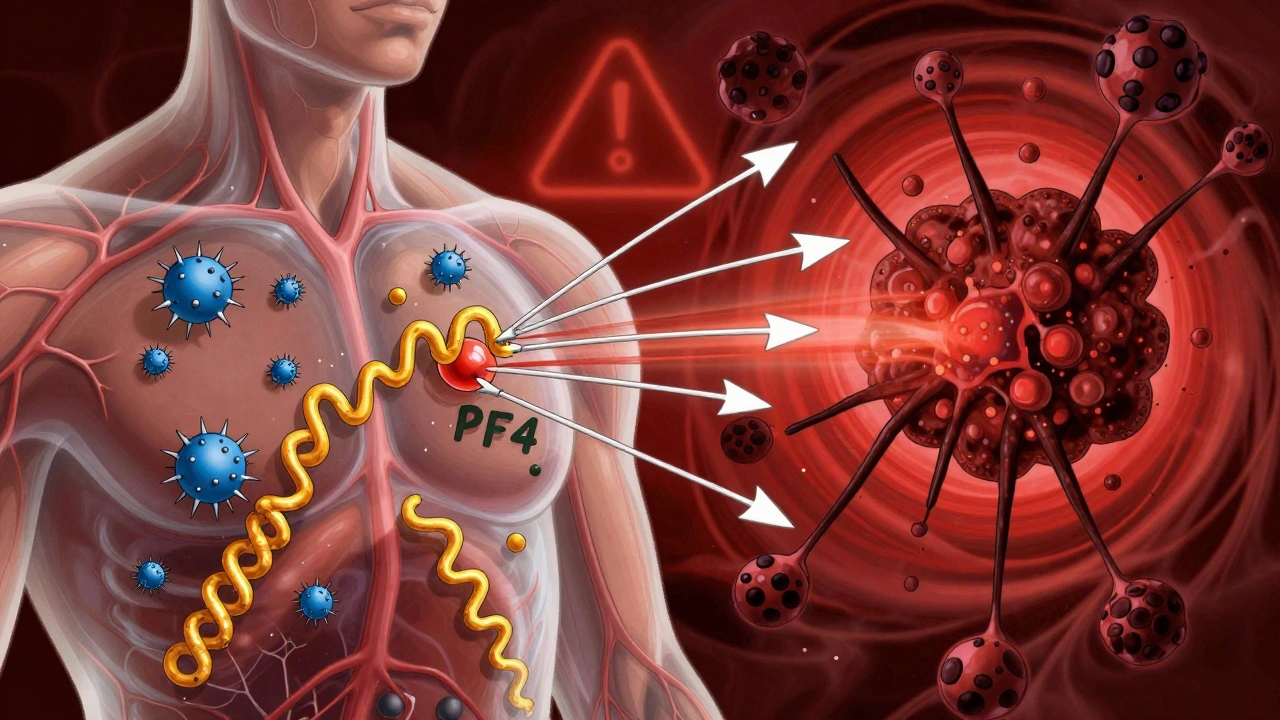
HIT isn't just a drop in platelets. It's a paradox. Heparin, a drug meant to stop clots, ends up causing them. This happens because your immune system mistakenly attacks a complex formed between heparin and a protein in your blood called platelet factor 4 (PF4). Antibodies bind to this complex, overactivating your platelets. They clump together and get used up - that's why your platelet count drops. At the same time, they release chemicals that turn your blood into a clotting machine. There are two types of HIT. Type I is mild and harmless. It shows up within the first two days, platelets dip a little, then bounce back on their own. No treatment needed. Type II is the real danger. That's the immune-driven form. It takes 5 to 14 days to show up after starting heparin. If you've had heparin in the last 100 days, it can hit in as little as 24 hours. That's because your body still has the antibodies from before.Who's at Risk?
Not everyone gets HIT. But some groups are far more likely to. Women are 1.5 to 2 times more likely than men. People over 40 face a 2 to 3 times higher risk than younger patients. But the biggest red flag? Surgery - especially orthopedic surgery. After a hip or knee replacement, up to 10% of patients develop HIT. That’s way higher than the 1-3% seen in medical patients. The type of heparin matters too. Unfractionated heparin - the older, more common version - carries a 3-5% risk. Low molecular weight heparin (like enoxaparin) is safer, but still risky at 1-2%. Even heparin flushes in IV lines or heparin-coated catheters can trigger it. About 15-20% of HIT cases come from these small, seemingly harmless exposures. The longer you're on heparin, the higher your risk. Less than 5 days? Risk is under 0.5%. Between 5 and 10 days? Risk jumps to 3-5%. Beyond 10 days? It hits 5-10%. That’s why doctors check platelet counts every 2-3 days starting on day 4 - right when the danger window opens.What Does HIT Feel Like?
Symptoms don’t always show up the same way. But if you're on heparin and suddenly feel something off, pay attention. The most common sign? A new blood clot. About half of HIT patients develop deep vein thrombosis (DVT) - swelling, warmth, pain in the leg. Or a pulmonary embolism (PE) - sudden shortness of breath, chest pain, fast heartbeat. These aren’t rare side effects. They’re the rule, not the exception. Skin changes are a major red flag. Around 10-15% of patients see dark, bruised, or blackened patches where heparin was injected. Sometimes, fingers, toes, or even nipples turn blue or cold. This is called acral ischemia - tissue dying from blocked blood flow. It’s a medical emergency. Other signs include fever, chills, dizziness, sweating, or unexplained anxiety. One patient described feeling like she was having a heart attack - chest pain, breathlessness - just hours after noticing her calf was warm and swollen. That’s not coincidence. That’s HIT.
How Is It Diagnosed?
You can’t diagnose HIT by symptoms alone. Too many things cause low platelets or clots. That’s why doctors use the 4Ts score - a simple checklist that looks at four things:- Thrombocytopenia - how low are your platelets? (Did they drop by more than 50%?)
- Timing - when did the drop happen? (5-14 days after starting heparin?)
- Thrombosis - are there new clots? (DVT, PE, skin necrosis?)
- Other causes - could something else explain it? (Infection, drugs, DIC?)
What Happens If It’s Not Treated?
Untreated HIT with clots has a 20-30% death rate. That’s not a small risk. It’s catastrophic. Survivors often face long-term damage - amputations, chronic lung problems from PE, or permanent nerve damage from blocked blood flow. About 5-10% of severe cases end in limb loss. And here’s the worst part: if you're given warfarin (like Coumadin) during an active HIT episode, it can cause skin necrosis - your skin starts dying in patches. That’s why you never start warfarin alone during HIT. You need to wait until your platelets are back above 150,000 and you're already on a safe alternative anticoagulant for at least 5 days.
How Is HIT Treated?
Step one: Stop all heparin. Every bit. That includes flushes, heparin-coated catheters, even heparin locks on IV lines. Just one drop can make things worse. Step two: Start a non-heparin blood thinner. There are four main options:- Argatroban - given through IV. Used if you have liver problems. Dose adjusted based on blood tests.
- Bivalirudin - also IV. Preferred in heart surgery patients.
- Fondaparinux - shot under the skin once a day. Now recommended as first-line for non-life-threatening cases. It’s effective in 92% of cases.
- Danaparoid - available in some countries. Not in the U.S.
What About the Future?
Scientists are working on better ways to catch HIT early. New tests that look only at PF4 antibodies - not the heparin-PF4 combo - could cut false positives from 15% down to 5%. That means fewer people get wrongly diagnosed and put on risky drugs. There’s also research into new anticoagulants that don’t interact with PF4 at all. Two candidates are already in Phase II trials. If they work, we might one day have blood thinners that don’t carry this hidden danger. But right now, the best defense is awareness. If you're on heparin, know the signs. If you're a healthcare provider, check platelets every few days. Use the 4Ts score. Don’t wait for perfect tests. Act fast. Because in HIT, time isn’t just money - it’s life.Living With HIT
If you’ve had HIT, you’ll never forget it. Many patients report lasting anxiety - not just about clots, but about future medical care. “Will I ever be able to get heparin again?” “What if I need surgery?” “Can I be safely anticoagulated?” The answer is yes - but you need to be careful. You’ll always carry a warning: you’ve had HIT. That means no more heparin, ever. Even a single flush can trigger a relapse. When you go to the hospital, tell every doctor, nurse, and pharmacist. Write it on your medical alert bracelet. Keep a card in your wallet. You may need long-term anticoagulation. Some people take fondaparinux or warfarin for years. Others switch to direct oral anticoagulants (DOACs) like rivaroxaban or apixaban - but only after careful review. These drugs don’t cause HIT, but there’s limited data on their use in HIT survivors. Your doctor will weigh the risks. The emotional toll is real. One patient said, “I survived the clot, but the fear never left.” Support groups and counseling help. So does knowing the facts. HIT is rare. But it’s real. And if you know the signs, you can stop it before it stops you.Can you get HIT from a heparin flush?
Yes. Even small amounts of heparin - like the flushes used to keep IV lines open - can trigger HIT. About 15-20% of HIT cases come from these low-dose exposures. That’s why hospitals now avoid heparin flushes in high-risk patients and use saline instead.
Is HIT the same as DIC?
No. DIC (disseminated intravascular coagulation) is a different condition where the body uses up clotting factors and platelets due to severe infection, trauma, or cancer. HIT is an immune reaction triggered specifically by heparin. While both cause low platelets and clots, the causes, timing, and treatments are different.
Can HIT happen again if I get heparin later?
Yes - and very quickly. If you’ve had HIT before, your body remembers the antibodies. Re-exposure to heparin within 100 days can cause HIT within 1-3 days. Even after a year, the risk remains. You must avoid all heparin products for life.
Do all blood thinners cause HIT?
No. Only heparin and its derivatives (like low molecular weight heparin) cause HIT. Direct oral anticoagulants (DOACs) like apixaban, rivaroxaban, and dabigatran do not trigger HIT. They’re safe alternatives for people with a history of HIT.
Why is HIT called a "paradoxical" reaction?
Because heparin is given to prevent blood clots, but in HIT, it causes them. You get low platelets (which sounds like a bleeding risk) but end up with dangerous clots instead. That’s the paradox - the drug meant to stop clotting ends up making it worse.
Christian Landry
December 9, 2025 AT 12:33Katie Harrison
December 10, 2025 AT 08:02George Taylor
December 12, 2025 AT 06:42Chris Marel
December 14, 2025 AT 04:38William Umstattd
December 15, 2025 AT 00:03Elliot Barrett
December 15, 2025 AT 10:56Maria Elisha
December 16, 2025 AT 17:34Tim Tinh
December 17, 2025 AT 07:42Olivia Portier
December 17, 2025 AT 20:30Tiffany Sowby
December 19, 2025 AT 06:22Asset Finance Komrade
December 19, 2025 AT 06:50Jennifer Blandford
December 19, 2025 AT 22:08Brianna Black
December 21, 2025 AT 06:24Shubham Mathur
December 22, 2025 AT 18:28