 May, 5 2026
May, 5 2026
You wake up with a sharp ache in your shoulder or knee. It hurts to lift your arm, kneel on the floor, or even roll over in bed. Is it just muscle soreness from yesterday’s workout, or is something deeper going wrong? For millions of people, this nagging pain signals bursitis or tendinitis, two common conditions that cause significant discomfort but are often confused.
Understanding the difference between these two types of joint inflammation isn’t just academic-it changes how you treat the pain. Treating bursitis like tendinitis can lead to weaker tissues and longer recovery times. The American College of Rheumatology notes that misdiagnosis leads to inappropriate treatment in nearly half of chronic cases, extending symptom duration by weeks. This guide breaks down exactly what happens inside your joints, how to spot the specific signs of each condition, and the most effective ways to get back to moving without pain.
Anatomy of the Pain: Bursae vs. Tendons
To understand why these conditions hurt differently, you need to know what structures are involved. Your joints rely on two key support systems: bursae and tendons. They work together to keep movement smooth, but they serve very different purposes.
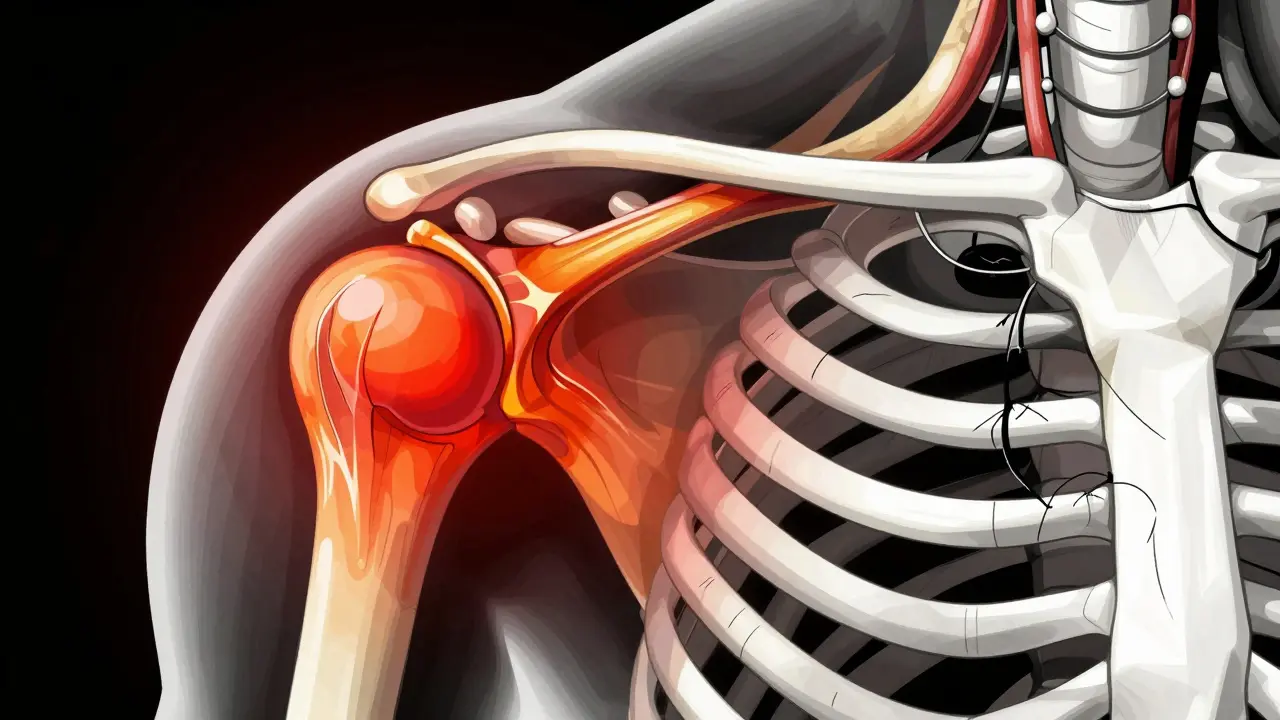
Bursae are small, fluid-filled sacs located throughout the body-there are about 160 of them. Think of them as biological ball bearings. Their job is to cushion bones, tendons, and muscles near joints so they don’t rub against each other. When a bursa becomes inflamed, it swells with excess fluid, causing pressure and pain. This is called bursitis.
Tendons, on the other hand, are thick, fibrous cords that attach muscle to bone. They act like cables, transmitting force so you can move. When a tendon gets irritated due to overuse or strain, it develops micro-tears and inflammation. This condition is known as tendinitis. While both involve inflammation, the structural damage in tendinitis is often more complex than the fluid buildup in bursitis.
| Feature | Bursitis | Tendinitis |
|---|---|---|
| Affected Structure | Bursa (fluid-filled sac) | Tendon (muscle-to-bone connector) |
| Pain Type | Dull, achy, diffuse around joint | Sharp, localized along tendon path |
| Trigger | Pressure, repetitive friction, trauma | Overuse, sudden increase in activity |
| Common Locations | Shoulder, elbow, knee, hip | Achilles, rotator cuff, patellar tendon |
| Primary Treatment Focus | Reducing inflammation and pressure | Strengthening tissue and eccentric loading |
Recognizing the Symptoms: Where Does It Hurt?
The location and nature of your pain are the biggest clues to whether you’re dealing with bursitis or tendinitis. While there is overlap, especially in the shoulder where subacromial bursitis and rotator cuff tendinitis often coexist, distinct patterns usually emerge.
Bursitis symptoms tend to be more generalized. You might feel a deep ache around the joint that worsens when you apply direct pressure. For example, if you have olecranon bursitis ("student's elbow"), lying your elbow on a hard desk will trigger immediate pain. Prepatellar bursitis ("housemaid's knee") causes visible swelling at the front of the knee after prolonged kneeling. Night pain is also common; many patients report waking up because lying on the affected side compresses the inflamed bursa.
Tendinitis symptoms are more mechanical. The pain follows the line of the tendon. If you have Achilles tendinitis, the pain is specifically at the back of the heel or ankle, not spread across the entire foot. Crucially, tendinitis pain is often worst during the first few steps in the morning or immediately after starting an activity, then may ease slightly before returning later. Dr. Robert Simkin of Brigham and Women’s Hospital notes that tendinitis pain is elicited by specific movements that stress the tendon, whereas bursitis pain is elicited by pressure on the bursa itself.
- Shoulder: Subacromial bursitis causes pain when lifting the arm overhead or lying on the side. Rotator cuff tendinitis hurts during specific lifting motions, especially reaching behind the back.
- Knee: Patellar tendinitis ("jumper's knee") hurts right below the kneecap during jumping or squatting. Prepatellar bursitis causes swelling directly over the kneecap.
- Hip: Trochanteric bursitis causes sharp pain on the outside of the hip, worse when sleeping on that side. Gluteal tendinitis hurts during climbing stairs or standing up from a chair.

Why It Happens: Causes and Risk Factors
Both conditions stem from repetitive stress, but the triggers differ slightly based on anatomy. Age plays a major role, with prevalence peaking between ages 45 and 64 according to the Framingham Osteoarthritis Study. As we age, tendons lose elasticity and bursae become less resilient to friction.
Repetitive Motion: Jobs or hobbies involving repeated movements are prime culprits. Construction workers often develop prepatellar bursitis from kneeling. Professional musicians face high rates of tendinitis in their hands and wrists due to precise, repetitive finger movements. Even office workers can develop lateral epicondylitis (tennis elbow) from improper mouse use.
Sudden Increases in Activity: Jumping into a new exercise routine too quickly is a classic cause of tendinitis. The tendon cannot adapt as fast as the muscle, leading to micro-tears. This is why "weekend warriors" frequently suffer from Achilles or patellar tendinitis.
Direct Trauma: A fall onto an elbow or knee can cause acute bursitis. The impact damages the bursa lining, causing it to fill with blood or fluid rapidly. This is less common for tendinitis, which is rarely caused by a single blow unless it results in a tear.
Underlying Conditions: Inflammatory diseases like rheumatoid arthritis or gout can predispose you to bursitis. Gout crystals can deposit in bursae, triggering severe inflammation. Diabetes has also been linked to slower healing in tendinopathy, making conservative management more challenging.
Diagnosis: Beyond the MRI
When you visit a doctor, the diagnosis starts with a physical exam, not imaging. Dr. Laura Robbins of the Hospital for Special Surgery warns that 40% of asymptomatic adults over 50 show signs of bursitis or tendinitis on MRI scans without having any pain. Imaging alone doesn't confirm the source of your suffering.
Physicians look for specific signs:
- Palpation: Pressing on the area. Bursitis is tender directly over the bursa. Tendinitis is tender along the tendon's path.
- Range of Motion: Moving the joint through its full range. Tendinitis often limits movement due to pain during contraction. Bursitis may allow full movement but hurt at extreme angles.
- Resisted Movement: Asking you to push against resistance. Weakness or pain during resisted motion suggests tendinitis.

Treatment Strategies: Rest, Inject, or Strengthen?
The treatment path diverges significantly depending on the diagnosis. Using the wrong approach can delay healing or cause harm.
Conservative Management (First Line): For both conditions, the initial step is similar. The American Physical Therapy Association recommends rest, ice, compression, and elevation (RICE) for 7-10 days. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can reduce pain and inflammation, but should be limited to 10-14 days to avoid gastrointestinal issues.
- Activity Modification: Avoid the specific movements that trigger pain. If kneeling hurts, use a pad. If typing hurts, adjust your workstation height.
- Ice Therapy: Ice massage is highly rated by patients. Rolling a frozen water bottle over the painful area for 10-15 minutes reduces local inflammation.
Physical Therapy and Eccentric Exercises: This is the gold standard for tendinitis. Unlike bursitis, which often resolves with rest, tendinitis requires active rehabilitation. Eccentric exercises involve lengthening the muscle under load. For Achilles tendinitis, the Alfredson protocol involves heel drops on a step, focusing on the lowering phase. This strengthens the tendon and remodels collagen fibers. Patients typically see sustained improvement after 12-16 weeks of consistent practice.
Emerging Therapies: Platelet-rich plasma (PRP) therapy shows promise for chronic tendinitis, with 67% improvement at 6 months compared to 42% for corticosteroids. While more expensive ($850 per injection), PRP uses your own blood components to promote healing. Extracorporeal shockwave therapy is also gaining traction for plantar fasciitis and other tendinopathies, offering pain reduction without invasive procedures.
Prevention and Long-Term Management
Once you’ve recovered, preventing recurrence is crucial. Both conditions thrive on neglect and poor mechanics.
- Gradual Progression: Increase activity intensity by no more than 10% per week. This allows tendons and bursae to adapt to new stresses.
- Proper Technique: Whether lifting weights, playing tennis, or digging in the garden, correct form reduces shear forces on tendons and friction on bursae.
- Flexibility and Strength: Tight muscles pull on tendons, increasing tension. Regular stretching and strengthening of opposing muscle groups maintain balance around the joint.
- Ergonomics: Adjust your workspace. Use ergonomic tools that fit your hand naturally. Take frequent breaks to change positions and avoid static loading.
Listen to your body. The "pain monitoring rule" suggests staying below 3/10 pain during rehabilitation exercises. Sharp, stabbing pain is a sign to stop. Dull discomfort is acceptable. Ignoring early warning signs turns minor irritation into chronic disability.
How long does it take for bursitis or tendinitis to heal?
Bursitis often resolves within 4-6 weeks with rest and anti-inflammatories. Tendinitis takes longer, typically requiring 12-16 weeks of structured physical therapy. Chronic cases can persist for months if not treated correctly.
Can I exercise with bursitis or tendinitis?
Yes, but you must modify activities. Avoid movements that cause sharp pain. For tendinitis, eccentric strengthening exercises are beneficial. For bursitis, gentle range-of-motion exercises prevent stiffness while avoiding pressure on the inflamed bursa.
Are cortisone injections safe for tendinitis?
Cortisone injections are generally safer for bursitis. For tendinitis, they offer limited long-term benefit and can weaken the tendon, increasing rupture risk. Use them sparingly and only under medical supervision.
What is the difference between tendinitis and tendinopathy?
Tendinitis implies active inflammation. Tendinopathy refers to degenerative changes in the tendon without significant inflammation, common in chronic cases. Many long-term "tendinitis" cases are actually tendinopathy, requiring different treatment approaches focused on load management rather than anti-inflammatories.
When should I see a doctor for joint pain?
See a doctor if pain persists beyond 2 weeks despite home care, if you experience significant swelling, redness, or warmth, or if you cannot bear weight on the affected limb. Early diagnosis prevents chronic issues.