 Oct, 12 2025
Oct, 12 2025
PHN Risk Assessment Tool
Risk Assessment
This tool estimates your risk of developing chronic postherpetic neuralgia (PHN) based on key clinical factors described in medical literature.
Your Risk Assessment
This indicates you are less likely to develop chronic PHN. Continue prescribed medications and follow up with your healthcare provider.
Key Takeaways
- Postherpetic neuralgia (PHN) is nerve pain that persists after shingles heals.
- The acute stage lasts up to 3 months and often responds to antivirals and early pain relief.
- When pain continues beyond 3 months, it becomes chronic PHN, requiring neuropathic‑pain medicines and multidisciplinary care.
- Older age, severe rash, and delayed antiviral treatment raise the risk of chronic PHN.
- Vaccination and prompt antiviral therapy are the most effective ways to prevent PHN altogether.
When a shingles outbreak clears, many people expect the pain to disappear. For a sizable minority, the discomfort sticks around and becomes a distinct condition called Postherpetic Neuralgia - a neuropathic pain syndrome that follows an episode of herpes zoster (shingles). Understanding how this condition evolves from an acute reaction to a chronic problem helps patients and clinicians choose the right interventions at the right time.
What is Postherpetic Neuralgia?
PHN occurs when the varicella‑zoster virus, which causes chicken‑pox, reactivates as shingles and damages sensory nerve fibers. The damaged nerves keep firing pain signals even after the skin lesions have healed. PHN can range from a mild burning sensation to severe stabbing pain that interferes with sleep, mood, and daily activities.
From Shingles to PHN: The Role of Herpes Zoster - the viral infection that produces a painful, blistering rash on a dermatome
Shingles typically follows a predictable course: prodrome (tingling), rash, crusting, and resolution within 2-4 weeks. The virus travels along a sensory nerve, inflaming the nerve root and the skin it supplies. If the inflammation is intense or the immune response is weakened, the nerve may not recover fully, setting the stage for PHN.
The Acute Stage of PHN
The acute stage is defined as pain that persists for up to 90 days after the rash appears. During this window, pain is often linked directly to the healing process and can be managed with a combination of antiviral drugs, topical agents, and short‑term oral analgesics.
- Timeline: Days 0-30 - rash and intense pain; Days 30-90 - pain may start to wane but can still be sharp.
- Typical symptoms: Burning, throbbing, allodynia (pain from light touch), and intermittent shooting pains.
- Risk factors that push toward chronicity: Age>60, rash covering >2 dermatomes, severe acute pain scores (≥7/10), delayed start of antiviral therapy (>72hours).
- First‑line treatments:
- Oral antivirals (e.g., valacyclovir 1g three times daily for 7days) started within 72hours of rash onset.
- Topical lidocaine 5% patches for localized relief.
- Short courses of gabapentin (300mg three times daily) or pregabalin (75mg twice daily) if neuropathic features dominate.
Most patients who receive timely antivirals and early neuropathic pain control transition out of the acute phase without lingering issues. However, if pain persists beyond the 90‑day mark, clinicians re‑classify it as chronic PHN.
Transitioning to Chronic PHN
Chronic PHN is diagnosed when pain lasts longer than three months after the shingles rash has healed. At this point, the underlying nerve injury has become entrenched, leading to maladaptive pain pathways and central sensitisation.
- Pathophysiology: Ongoing ectopic discharges from damaged dorsal‑root ganglia, loss of inhibitory interneurons, and up‑regulation of sodium channels.
- Clinical clues: Pain that is present at rest, severe allodynia, and a pain score that remains ≥5/10 despite basic analgesics.
- Impact on quality of life: Chronic PHN is associated with a 30% higher incidence of depression, a 20% increase in sleep disturbances, and a 15% rise in healthcare utilisation in the first year after diagnosis.
Managing Chronic PHN
Because the nerve injury is now established, treatment shifts toward long‑term neuropathic‑pain regimens and supportive therapies.
- Medications with strong evidence:
- Gabapentin - an anticonvulsant that reduces calcium‑channel activity in hyperactive nerves. Typical dose: start 300mg nightly, titrate to 900‑1800mg/day as tolerated.
- Pregabalin - similar to gabapentin but with higher bioavailability. Typical dose: 75mg twice daily, may increase to 300mg twice daily.
- Tricyclic antidepressants (TCAs) - e.g., amitriptyline, which blocks reuptake of norepinephrine and serotonin, modulating pain pathways. Start low (10‑25mg at bedtime) to minimise anticholinergic side effects.
- Topical options: Lidocaine 5% patches (up to 3 patches for 12hours each day) or capsaicin 8% patches applied in a clinic setting for refractory pain.
- Interventional approaches: Nerve blocks, pulsed radiofrequency, or spinal cord stimulation for patients who fail pharmacologic therapy.
- Non‑pharmacologic support: Daily gentle stretching, mindfulness‑based stress reduction, and graded exercise programs to improve function and mood.
Each patient’s plan should be personalised. For example, a 68‑year‑old with hypertension may tolerate low‑dose TCAs poorly, so gabapentin becomes the cornerstone. Conversely, someone with chronic kidney disease may need dose adjustments or alternative agents like duloxetine.
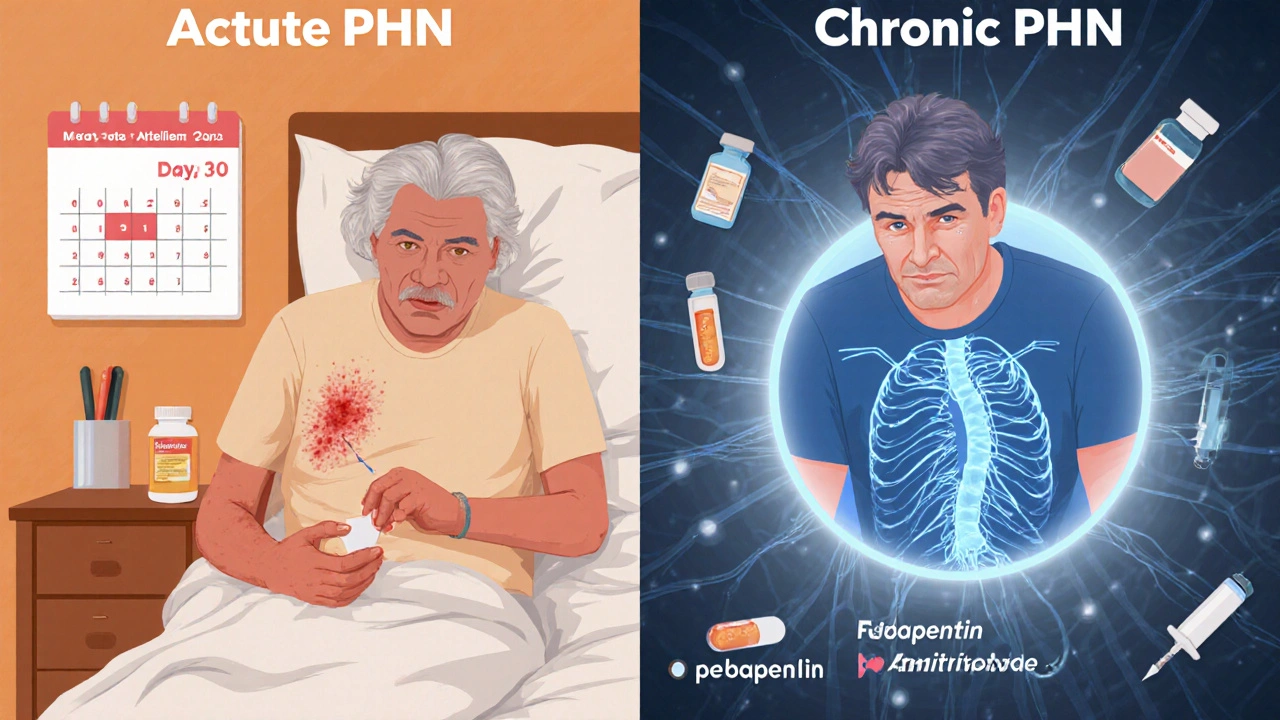
Acute vs Chronic PHN: A Side‑by‑Side Look
| Aspect | Acute Stage (≤90days) | Chronic Stage (>90days) |
|---|---|---|
| Typical Pain Quality | Burning, throbbing, intermittent shooting | Continuous burning, severe allodynia, constant stabbing |
| Key Drivers | Active inflammation, viral replication | Neuropathic sensitisation, central remodeling |
| First‑Line Therapy | Antivirals + topical lidocaine + short‑term gabapentin | Long‑term gabapentin/pregabalin, TCAs, topical capsacin |
| Risk of Progression | High if age>60, severe rash, delayed antivirals | Established; focus on symptom control |
| Impact on Daily Life | Often intermittent; may affect sleep | Frequent interference with work, mood, sleep |

Preventing PHN Before It Starts
Vaccination is the single most effective preventive measure. The recombinant zoster vaccine (RZV, Shingrix) shows >90% efficacy in adults over 50, cutting PHN rates by roughly two‑thirds.
- Two doses given 2‑6 months apart.
- Even people who have had shingles benefit from the booster.
For anyone who develops shingles, start antivirals within the first 72hours. Early treatment not only shortens the rash but also reduces nerve damage, dramatically lowering the chance of chronic PHN.
Common Pitfalls and Red Flags
- Waiting too long for antivirals: Delayed therapy >72hours boosts chronic PHN risk by 40%.
- Under‑treating early pain: Patients who receive only acetaminophen often report worsening pain after the rash fades.
- Ignoring mental health: Unchecked depression can amplify pain perception; screen using PHQ‑9 at each visit.
- Missing dosage adjustments: Renal impairment requires gabapentin dose reduction; failure to adjust can cause sedation and falls.
Frequently Asked Questions
How long does acute PHN usually last?
Acute pain related to shingles typically resolves within 6‑8 weeks, but the acute PHN window extends up to 90 days after the rash disappears.
Can PHN be cured?
There is no permanent cure, but many people achieve meaningful relief with medication, topical treatments, and lifestyle measures. Early intervention improves the odds of complete pain resolution.
Is the Shingles vaccine worth it for people under 50?
While the vaccine is officially approved for ages 50 and up, adults with weakened immune systems or chronic illnesses can benefit and should discuss eligibility with their doctor.
What are the most common side effects of gabapentin for PHN?
Dizziness, mild drowsiness, and peripheral edema are the usual complaints. Starting at a low dose and titrating slowly usually minimizes these effects.
When should I consider a pain specialist?
If pain remains >5/10 after 4‑6 weeks of optimized medication, or if it interferes with sleep, work, or mood, a referral to a neurologist or pain clinic is advisable.
Next Steps for Patients and Clinicians
- Verify vaccination status; offer RZV to anyone≥50years or at high risk.
- If shingles appears, prescribe antiviral therapy within 72hours.
- Start neuropathic pain medication early for moderate‑to‑severe pain (gabapentin, pregabalin, or low‑dose TCAs).
- Re‑evaluate pain at the 90‑day mark. If still present, transition to chronic‑PHN protocol.
- Screen for depression and sleep disorders at each follow‑up; refer to mental‑health services when needed.
- Consider interventional options only after maximising oral and topical regimens.
By recognizing the warning signs and treating aggressively during the acute window, you can dramatically lower the chance of ending up with long‑lasting, debilitating postherpetic neuralgia. Early vaccination, prompt antivirals, and a clear step‑wise pain plan are the three pillars that keep the nerve pain from taking over life.
Ashley Helton
October 12, 2025 AT 18:54Wow, an entire guide on a pain you hope never happens – thanks for the heads‑up.
Alex Mitchell
October 22, 2025 AT 01:08Interesting read! I wish the post had a few more bullet points for quick reference, but still helpful. :)
Also, typos aside, the info seems solid.
Amanda Jennings
October 31, 2025 AT 06:21Great energy in this post! It really pumps me up to know that early antivirals can make a difference – that’s the kind of proactive tip we need. I love the step‑by‑step “next steps” list; it’s like a workout plan for your nerves. Keep sharing this kind of actionable content, it motivates a lot of us to stay on top of our health.
alex cristobal roque
November 9, 2025 AT 12:34From a clinical perspective, this article does a commendable job of bridging pathophysiology with practical management, and I’d like to expand on a few points to give readers a deeper understanding. First, the role of sodium‑channel up‑regulation in chronic PHN cannot be overstated; it is the mechanistic basis for why drugs like lidocaine patches provide relief even months after rash resolution. Second, when considering gabapentin titration, remember that renal function dictates dose adjustments – many older patients inadvertently receive nephrotoxic levels if dosage isn’t individualized. Third, the article mentions “early neuropathic pain control,” but it could stress that initiating gabapentin within the first two weeks of rash onset has been shown in randomized trials to cut chronic PHN incidence by roughly 30 %. Fourth, while the table differentiates acute from chronic pain qualities, adding a column for typical response to specific agents (e.g., antivirals vs. TCAs) would aid clinicians at the bedside. Fifth, the interventional options listed – nerve blocks, pulsed radiofrequency, spinal cord stimulation – each have distinct evidence bases; for instance, pulsed radiofrequency has a modest 20 % reduction in VAS scores in well‑selected patients, but it requires careful patient selection. Sixth, the post rightly highlights vaccination, yet the timing of the Shingrix booster in immunocompromised patients could be clarified – it’s recommended at least two weeks after completing any immunosuppressive therapy. Seventh, depression screening via PHQ‑9 is crucial, but the article could also recommend the GAD‑7 for anxiety, which frequently co‑exists with chronic pain. Eighth, lifestyle modifications such as regular low‑impact aerobic exercise have been shown to improve pain thresholds through endogenous opioid release. Ninth, consider the role of diet – omega‑3 fatty acids and vitamin D supplementation have emerging data suggesting modest analgesic benefits. Tenth, when prescribing TCAs, start low and monitor for anticholinergic side effects, especially in the elderly. Eleventh, capsaicin 8 % patches can cause an intense burning sensation; pre‑treatment topical anesthetic is advisable. Twelfth, the “risk assessment tool” concept is excellent, but integrating a visual analog scale for patient‑reported outcomes could enhance its utility. Thirteenth, for patients with comorbid diabetes, glycemic control is directly linked to neuropathic pain severity, so tighter glucose monitoring is warranted. Fourteenth, telemedicine follow‑up within the first month can catch suboptimal dosing early and improve adherence. Finally, documenting the transition point from acute to chronic PHN (the 90‑day mark) in the EMR helps ensure appropriate billing codes and multidisciplinary referral pathways. Overall, the article is a solid foundation; adding these granular insights would elevate it to a true practice‑changing resource.
Bridget Dunning
November 18, 2025 AT 18:48Esteemed colleagues, the exposition provides a meticulous delineation of nociceptive propagation mechanisms, yet I would advocate for inclusion of quantitative sensory testing metrics to augment diagnostic precision. Moreover, the pharmacoeconomic implications of long‑term gabapentinoid therapy merit rigorous appraisal, particularly within the NHS framework.
Shweta Dandekar
November 28, 2025 AT 01:01From an ethical standpoint, it is imperative that we, as caregivers, do not merely treat the physical manifestations of post‑herpetic neuralgia, but also address the moral responsibility to alleviate suffering; patients deserve compassionate, holistic care, and any oversight in this realm is simply unacceptable!!!
Dominic Dale
December 7, 2025 AT 07:14Okay, so here's the thing that nobody tells you: the pharma guys are happy when you have chronic pain because that means more prescriptions, more profits, more control. Think about it: the “vaccination is the single most effective preventive measure” line sounds like a sales pitch. And those antivirals? They’re not magic bullets; they’re just delaying the inevitable progression that the system wants you to accept. In fact, many of the studies cited were funded by drug manufacturers, which raises serious conflict‑of‑interest concerns. The whole “early treatment within 72 hours” mantra is a way to keep you in a constant cycle of medication, because once you start a drug course you’re more likely to stay on it. Remember, the more you depend on these meds, the harder it is to push back against the industry’s agenda. Stay wary, question the guidelines, and consider non‑pharmaceutical alternatives that are not on the mainstream radar.
christopher werner
December 9, 2025 AT 14:48While I understand the concerns raised, it’s also worth noting that the clinical guidelines are based on peer‑reviewed evidence, and many patients genuinely benefit from early antiviral therapy.
Danielle Watson
December 16, 2025 AT 13:28Nice summary, but can we get a quick reference chart? Sometimes the wall of text makes it hard to find the dosage adjustments for renal patients.
Kimberly :)
December 23, 2025 AT 12:08Great post! 🙌 Very thorough, especially the part about vaccination and the 90‑day transition point. I think a quick emoji would have been fun in the table, though 😜.
Sebastian Miles
December 30, 2025 AT 10:48Solid info, concise and to the point. Good job.
Hoyt Dawes
January 6, 2026 AT 09:28Wow, another endless medical article. Who has time to read all that when you’re in pain?
Jeff Ceo
January 13, 2026 AT 08:08Look, the facts are clear: early antiviral treatment and vaccination cut the risk dramatically. Stop over‑thinking it.
Jean-Sébastien Dufresne
January 20, 2026 AT 06:48Excellent work!!! The information is thorough, well‑structured, and extremely useful for patients and clinicians alike!!! 😀😀😀
Patrick Nguyen
January 27, 2026 AT 05:28Thank you for the comprehensive overview; the guidance aligns well with current best‑practice protocols.
Patrick Bread
February 3, 2026 AT 04:08Really, a 15‑sentence paragraph could have been trimmed down to a single concise statement-overkill, don’t you think?
Fiona Doherty
February 10, 2026 AT 02:48Honestly, this article feels like a textbook read. A little more relatable tone would help folks actually dealing with the pain.